
 Diagnosing Mast Cell Activation Syndrome (MCAS) – Post 1 of 4 post series
Diagnosing Mast Cell Activation Syndrome (MCAS) – Post 1 of 4 post series

In early June 2015, I traveled to see Dr. Larry Afrin, one of the most recognized and published physicians on Mast Cell Disorders.
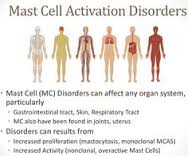
It’s important to first point out the difference between Mast Cell Activation Syndrome (MCAS) vs. other mast cell disorders, such as Mastocytosis. Mast Cell Activation Syndrome (MCAS) is one type of mast cell disorder under the Mast Cell Activation Disorder umbrella. Mastocytosis is another type of mast cell disorder; however, it varies from MCAS in that those with Mastocytosis have too many mast cells. Those with MCAS, have mast cells that are very sensitive and react too much. Symptoms are often similar between MCAS and Mastocytosis, but severity of the illness and treatments can vary depending on the actual diagnosis, or type of Mastocytosis. To read more go here.
I waited several months for this appointment, and honestly, I was reluctant to go for several reasons. I felt like: I’m walking, functioning and capable, so I should not take a spot from someone who is really sick. But my husband insisted and I’m very happy that he did. I needed to get answers, needed a more exact diagnosis based on personal and family history, as well as testing (that can really only be properly done here in MN) and Dr. Afrin is really the only one who can do it. I’ve exhausted all options available, close within my area (tried to get into NIH trial, have communicated with Dr. Theo and have trialed several meds) and my issues and reactions are nearly constant, as well as increasing in frequency.
The problem with Mast Cell Activation Disorders is that they can make you feel straight-up crazy. I knew I had mast cell issues, but I was never as severe as many who I help, or at least not until last year. Last October I got the flu shot for work and all heck broke loose. Things probably had been rocky for quite some time and I was definitely teetering on the edge of keeping things from going really haywire; however, the flu shot, along with Hashimoto’s Hypothyroidism not being well-regulated, is what did me in. Like I said, mast cell issues can make you feel like you are losing your mind and maybe you are, because mast cells and inflammation are in the brain too, and are a big component in psychiatric disorders. Symptoms can be so strange, irregular, yet constant, incredibly hard to explain, hard to understand and devastating. Sometimes it’s really hard to know what is going on.
THIS is my every day, multiple times a day now, when previously crazy reactions had only happened a few times a year and nothing this severe or complex. THIS is why I went to see Dr. Afrin, but I wasn’t really sure if there was enough history to give him what he needed. I felt like I fell in some category off to the side — someone with a lot of issues, but still functioning. I was willing to bet that even Dr. Afrin would not get my symptoms. However, my concerns couldn’t have been farther from the truth.
I brought all the medical records that I figured would help, but I was missing a lot – cardiology reports, years of eye doc appointments for weird allergic reactions and issues with my eyes, a lot of Dr. Pocinki’s notes and labs, records from the 2 visits to Suburban Hospital’s ER, endocrinology records & labs, pics of the rash in Mexico during college and most of my records for the past 2 years. Still, he found enough, and along with the timeline of my life (giving exact events, issues, etc.), Dr. Afrin stated that he had “plenty.”

Below is the gist of what I found out, both personally and about MCAS research (especially the overlaps with EDS). I should state that the following are not direct quotes from Dr. Afrin, but more me paraphrasing his answers to my questions, along with my own knowledge in order to provide more details and explanation. I think it’s also important to note that Dr. Afrin’s answers may be just his opinion based on his knowledge or experience thus far or based on research that has been accepted as fact for MCAS/MCAD, and/or specific to my case. I did not clarify which was which with him, because he spent a lot of time with me and I just appreciated him answering my questions. I tried to make sure that I stated theoretically, possibly, and other words that give an appropriate account of the information stated. It is not my intent to share this information so that we can see who agrees or disagrees, nor do I mean for it to be taken as my opinion of what someone else should do. My intent is to state my overall experience, why I almost didn’t go, and what I learned. We are all responsible for our own medical care and being our own healthcare advocate. The physicians who devote their lives to treating us, do the best they can, but they are also human, make mistakes and need a little understanding, just like the rest of us. None of this should be taken as a substitute for seeking medical care and counsel from your healthcare provider. This post was originally posted on SFHEDS.com and all posts (post -4), can be found by going here.
Once Dr. Afrin was finished reviewing my records and going through my timeline of life, he looked at me and said, “Well, what can I tell you that you already don’t know?” I took that as a good thing and just asked him to run through my list of questions with me and answer to the best of his knowledge and as he is comfortable.
1. Historically, my blood work has shown that RBCs and Hemoglobin have run somewhat high — I guess that’s been noted with other patients as well. The reason? Not sure, but it could help determine the right type of treatment and why one works for certain patients (or ones like me) and not others.

2. My previous GI and Chronic Pelvic Pain procedures also gave some insight, but I’m not sure what just yet other than Dr. Afrin’s office can contact the doctors and have the tissue samples stained for mast cell infiltration. Obviously this will help general research, and it helps determine if a bone marrow biopsy is warranted. Bone marrow biopsies are done in order to confirm or rule out the diagnosis of mastocytosis (in my case, indolent mastocytosis and even if I don’t have a high tryptase). However, Dr. Afrin does not feel that a bone marrow biopsy will be necessary in my case.

3. My personal medical history and clinical exam showed “classic” Mast Cell Activation Disorder (MCAS); however, Dr. Afrin will not give an exact dx until all tests come back. ALL. He also will not recommend any type of treatment, other than just doing a H1 & H2 combo like Zytrec and Zantac or Pepcid and Claritin until all tests are back. The first combo hasn’t worked for me, so I may try the 2nd and see if I can find some relief. I can only hope that I will be able to eat a bit more and not swell like a stuck pig, or be debilitated by horrible stomach pain and nausea.
4. Treatment for MCAS is just as personal and varied as each case of EDS. You may find relief on the 5th treatment option or the 1st or maybe the 15th. Just be prepared for the long-haul. He will continue to help find something that works and most patients do find something eventually.

5. Symptoms should get better with appropriate treatment. Which ones? Who knows, but he stated to not expect all symptoms to get better.
6. Diet – does help a lot of people, but Dr. Afrin would not say which “type” of dietary changes to do because we are all different. What works for one, will not work for 500 others. It is all trial and error, individually. However, we did discuss my voodoo drinks (AKA – Gouter tonics), what they are made of, what I found through drinking them, as well as from a mostly liquid diet and he didn’t react like my experience was totally off-base from what has worked for others.

7. Theoretically MCAS could turn to Mastocytosis, but that usually doesn’t happen. However, the general medical community still does not recognize MCAS as its own condition and refuses to see how common it really is (I said 10% of pop & Dr. Afrin said 7-17%). It’s been very hard to separate MCAS from Mastocytosis and thus, research money is limited and very hard to come by. This is why a dx with proper testing vs. a solely clinical dx can help all of us in the long run. However, I understand that most of us need to go to whoever understands MCAS in general and testing is not always accessible. I know it wasn’t for me and I was dx clinically up until now. Technically, I’m still not dx based on lab results. Medicine is evidence based and having lab tests that can prove why symptoms present clinically, will help show the greater medical community how not so rare MCAS is. Testing is documented and cannot be refuted as “just” someone’s personal interpretation of a patient’s symptoms. It can also show how varied we present and the more people with proper lab testing, the more attention paid to MCAS (this is my hunch from working in the medical community) and thus, the more money donated and granted for research. Testing will become more efficient and available if MCAS is recognized to be as common as Dr Afrin states. Pharmaceutical and research companies will also pay more attention because test results (genetic and lab tests) help find the underlying problem, and companies can find ways to develop treatments. I.e. Losartan is being looked into for the expression of the Marfan gene (Dr. Francomano – EDS UK one day conference 2015). Losartan is a BP medication and without testing (via genetic, pathological tests of symptoms & clinical evidence), I’m guessing that the link between Losartan and the Marfan gene expression would not have been researched.
8. Dr. Afrin discussed the idea of one main condition that is underlying for many of us — even for those who have EDS and MCAS. Why and what is it? He could only speculate, but this is where money for research is so important, because there are probably several different types of MCAS, just as it’s been noted recently that experts are looking at HEDS as having various “types” as well. Do some types of both conditions overlap and are actually one main cause/condition? Dr. Afrin seems to think it’s a good possibility. However, we need interest and money to research certain groups of people and that’s hard when the greater medical community doesn’t recognize MCAS and even EDS for what they really are, not to mention how prevalent. What complicates all of this even more? Epigenetics – see number 9.
9. Dr. Afrin talked a lot about epigenetics and how much they seem to play a part in both HEDS and MCAS. We know that environment, lifestyle and stress can change the way our genes are expressed (i.e. we inherit the same genetic mutation as our mom, but we are much more severely affected), but epigenetic changes to our own gene expression can consequently be passed down. Basically, we have infinite possibilities of how proper gene expression is affected. Just because of environmental stressors, or we’ve gone through trauma during our lifetime, or maybe we chose poor diet, and did not remain active most of our lives; our life experiences & choices do not occur in a vacuum. These life experiences and lifestyle choices are proving to not only affect expression of whatever genetic mutation(s) we originally inherited from our parents and the expression of our good genes during our lives, but also the expression of inherited mutations in our children. This is where research is showing how and why our own cases of MCAS or EDS (or both) quite possibly are more severe or not, than our own parents. Of course, this applies to many other heritable & lifestyle conditions and also goes along with the idea that we inherit a “predisposition” for certain conditions like diabetes or strokes, but lifestyle factors and environmental keep these genes turned off or switch them to “on” and activated in our bodies.
10. MCAS is theoretically linked to other hematological conditions – Mast Cell Activation Syndrome does increase your chance of developing other hematological conditions, but only research will be able to prove why and if there’s a higher chance with one condition over another. I asked about this because of my mom having amyloidosis and her father having sarcoidosis. amyloidosis is a blood/hematological condition and sarcoidosis involves abnormal growths, but both are cousins to each other and related to immune system function. Similarly, amyloidosis involves the same protein as Alzheimer’s and is a cousin to Multiple Myeloma. There’s no telling what a genetic mutation will do or could cause within someone’s body, because so many other factors affect that gene’s expression. There are countless scenarios that can play out and not all are lifestyle related or controllable (the environment that we work in or the family we were born into), yet they can affect various aspects of how our body functions and how it responds to stressors. (see number 10 above).

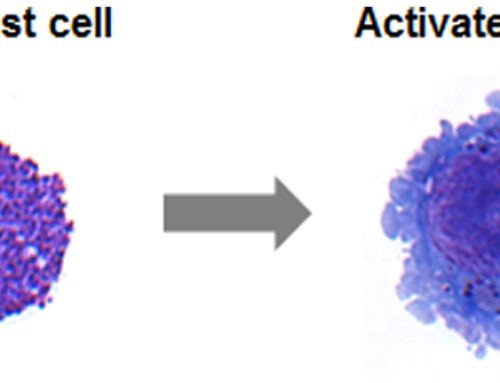
Graphic showing mast cell degranulation causing classic facial flushing and rash
11. Stress is by far the #1 trigger for MCAS. This could be trauma, physical stress from your body working too hard because it doesn’t have proper nutrients to sustain work, various lifestyle choices, the environment, or our own inborn nature of how we deal with change etc. Example – the natural fight or flight response to stress. This is associated with adrenaline rushes, dysautonomia and POTS, as many talk about. Stress affects the expression of the genes that help our mast cells function properly — this is epigenetics at its finest. If we inherited a mutation to our mast cells, or something that results in our mast cells constantly being triggered, the stress felt by our bodies has a direct connection to the symptoms we see and feel and can even possibly cause a new mutation to our inherited mutation.
Additionally, stress is not just what we feel during the fight or flight state. It is also stress that we don’t always see, hear, smell, feel or sense. The worst type, in my opinion, is the type of stress we have no idea our bodies are under. It’s the type we brush off; push back deep down and move on from, because it seems like no biggie. Many times, stress can trigger our mast cells and cause POTS/Dysautonomia or feelings of always being in the fight or flight state, but it can also go other way. These states and even the medications we take to help, can cause a much bigger problem than what we were trying to solve in the first place.
Learning how to respond to stress will help our bodies respond better, which will help our mast cells in the long-run. It takes time & lifestyle and behavior changes, because there are plenty of stressors we can’t control. We can only change the ones that we can control and ensure that we are paying attention to the not so obvious ones. I believe our bodies give us small clues that are many times not within the norm. This is a huge area for me with my health. It is often the stress that I don’t feel that triggers the symptoms I do feel. This issue then causes my body to respond and react to other things in my life that my body usually handles just fine (ie. a medication or a food), but does not when the quiet stress accumulates. These things are now viewed a stressors/”allergens” and my mast cells feel like they need to attack constantly. It’s funny, because I feel like I’ve been fighting to survive (figuratively not literally) in various ways over the last 4 years. However, it now seems that my body feels that same way and is responding as such.
Anaphylaxis is common in MCAS and MCAD; however, recognizing the various signs of anaphylaxis is critical. Stress can cause a vicious cycle of mast cell degranulation (i.e. triggered to release chemicals in response to a perceived threat). This is a quote taken from an article Cathy posted in her Mast Cell Research group, “Several lines of evidence indicate that stress, working through the sympathetic nervous system, or the hypothalamus-pituitary-adrenal axis, stimulates peripheral nerves to release neuropeptides that bind to receptors on the mast cells, causing them to degranulate. “

12. Link to Ehlers-Danlos Syndrome (EDS)? Dr. Afrin seems to think that there’s definitely a link, but finding the link will be up to research. He also seems to have theories, but did not elaborate much on a name of genes or research, other than stating that there are not enough studies being done on EDS patients with MCAS. I only know of one study personally and he didn’t seem to know of any, outside of his observations. However, research would have to examine various subgroups as I stated above and identify a common link.

Mast Cells in loose connective tissue – the most abundant type of connective tissue in our bodies.
I did ask about CBS gene & MTHFR mutations since I have read about both being studied for EDS and have read about links to MCAS, but he did not seem aware of the information. That doesn’t mean it isn’t happening, but he didn’t seem to be aware of it. He also did not think that either one was the cause of EDS or MCAS and could possibly be the opposite. Whatever is found to be the cause(s) of MCAS or even HEDS, could cause CBS gene or MTHFR issues. Again, this seems to be Dr. Afrin’s personal opinion, along with the fact that he also feels that there’s probably one main underlying condition for many of us that have both EDS and MCAS. He seems to believe the link between EDS and MCAS or the exact gene(s) causing both, may reside within an issue or mutation(s) that affects the way mast cells function — i.e. a protein, enzyme or anything. Again, both those who are studying EDS and Dr. Afrin have stated that there are probably a variety of types of HEDS and MCAS, but where the overlap is and if there is a certain set of mutations that cause both conditions or provides proof that some types of HEDS and MCAS are actually one in the same condition, will only be found through fairly detailed research (and we need money for that).
Personally, the way I look at it — mast cells are found all over our bodies and only reside in our connective tissues. They do not circulate in our peripheral blood unless traveling from our bone marrow to our tissues. Furthermore, our connective tissues are made up of several components including collagen, elastin, mast cells, other cells, etc. Any one issue that affects even just one component used to build our connective tissues, could affect the overall integrity. And according to my good friend Jan who runs one of the big MCAS/Masto groups, when you look-up Mast Cell/Mastocytosis in one of the old medical dictionaries, it’s called “Connective Tissue Disease.” The link seems pretty clear to me.images-11
13. Electronics can affect Mast cells – electronics can trigger mast cells, as can certain frequencies, types of light (i.e. ultraviolet, infrared) and other physical structures. Triggers are not always biological.
14. Mast Cells & inflammation of the brain have been found in association with every single psychiatric condition, yet the mainstream medical community does recognize the need for additional research in the association between psychiatric conditions & mast cell activation syndrome (or even mast cell activation disorders overall).
15. Mast Cell Disorders are the ultimate inflammatory conditions known.

16. Melasma & other skin issues can be connected to mast cell disorders. For me, these issues first started as what seemed like typical melasma or photo effects from sun damage, but anyone who knows me will agree that I’m compulsive about my face. I am rarely in the sun and take very good care of my skin, but despite efforts to lighten, laser and peel, skin issues on my face have become more pronounced. Specifically, my forehead has more light spots of discoloration and areas where the skin has a different texture. I also have areas near my chin that I had chronic small hives, which has thankfully gone away, but the issues on my forehead have remained. Due to changes in the dermis, some of my hair has fallen out and that doesn’t help someone who already has super blonde hair. I also noticed that the melasma and lighter spots would be more pronounced when I was in a flare, just like the dark circles under my eyes. To make matters worse, over the last few years, I noticed that even if my forehead has not seen the sun in months, the fact that I wear sunscreen daily and a hat when outside, if I did got outside or on the beach, my forehead would look as though I had been in the sun for months. Clearly whatever was going on was irritated by the heat and humidity and that’s when I knew it must be mast cell related. I don’t do well in heat and humidity and ended-up searching for links between Melasma and MCAS, as well as other dermatological changes. A few of my friends in the mast cell groups helped me find and verify my hunch. Dr. Afrin just confirmed it. I’ve also noticed that my skin has gotten more stretchy, not a ton and nothing that someone else would notice, but it’s definitely more extensible in the areas that someone would test for CEDS and it seems that the overall make-up of my skin has changed. It’s hard to explain, but I can see it and it’s clearly something that is related to this continued flare from mast cell activity. I did not ask Dr. Afrin this specific part about changes to the skin’s elasticity or over appearance, but I’m going off of connections I’ve made, research I’ve read and my overall conversation with Dr. Afrin.
17. Other pertinent information on MCAD, MCAS and anaphylaxis – Anaphylaxis has various stages and not everyone experiences the grade 4 or even 5. Recognizing that there are various grade of anaphylaxis is critical to finding proper treatment and help in an emergency situation.

18. The best news was that I was able to hand deliver Dr. Afrin a copy of Our Stories of Strength – Living with Ehlers-Danlos Syndrome. I also asked him if he would be willing to work with us on the MCAS/MCAD anthology and write the forward. He seemed genuinely interested and I’m excited at the prospect of working with him in the future. With that being said, anything can happen and anything can change. The physicians who treat us are incredibly busy and not everything works out as planned. None the less, we are incredibly excited and honored that he would even consider writing a forward for us.
This post was originally posted on SFHEDS.com. The original post can be viewed here. To read posts 2-4, see links below:
Diagnosing Mast Cell Activation Syndrome (MCAS) – Post 2 of 4 in series
Diagnosing Mast Cell Activation Syndrome (MCAS) – Post 3 of 4 in series
Diagnosing Mast Cell Activation Syndrome (MCAS) – Post 4 of 4 in series
Last, Our Stories of Strength is currently accepting submissions for the MCAS/Mastocytosis
anthology. To view the call for submissions page for the MCAS/Masto anthology, go here.
Resources for Mast Cell Activation Disorders:
– Anaphylaxis Emergency Information
– About Mast Cell Activation Disorder (and its subtypes) by Mast Attack.com
– Publication by Dr. Afrin – Mast cell activation disease: a concise practical guide for diagnostic workup and therapeutic options
– Dr. Afrin’s contact information in Minnesota
– EDNF Learning Conference Slides by Dr. Maitland
– EDS Awareness webinar recording by Dr.Maitland
– EDS Awareness webinar recording by Dr. Theo
– Dr. Theo’s website with various publications on mast cell activation disorders & relation to various other conditions, such as autism, interstitial cystitis, fibromyalgia and more. www.mastcellmaster.com.
Edits by Justine Case – wonderful friend, incredible writer, fellow EDNF HelpLine volunteer, and EDSers with MCAS.
DISCLAIMER: This information is for information purposes only. The above information and statements should NOT be construed as an endorsement for a physician mentioned on this website or in this post. You MUST do your own due diligence. This site accepts no liability WHATSOEVER if you consult any of the physicians named or those who I’ve personally seen, or medical care (or lack there of) in the event of a true medical emergency like anaphylaxis. Always seek the care of a physician concerning your health or any questions you have. If you have questions about anaphylaxis, go to: http://www.aaaai.org/conditions-and-treatments/allergies/anaphylaxis.aspx. This website and the four-post series originally posted on www.sfheds.com and is for your information ONLY. This information should not be viewed as a directive or as complete medical facts. You are responsible for your own health and well-being, as well as to do your own medical research. Please read additional information here.
{kind=link}
{kind=link}
{kind=link}